Groin pain can have a variety of pathologies. It’s extremely important to identify the root of the pain because the specific cause may drastically affect the appropriate treatment for pain relief and return to optimal athletic performance.
In case you’re late to the party and missed Part 1-5 of this comprehensive article series, you can view them here, here, here, here, and here.
Part 1: How non-contact injuries occur in sport and why well-functioning hips are necessary for elite ice hockey performance.
Part 2: Prevalence of hip injures in ice hockey, how and to whom they occur, with a special focus on groin strains.
Part 3: Review of where groin pain may actually be coming from (spoiler alert: it may not be from the groin muscles)
Part 4: The financial cost of injury for NHL players, and the potential costs to sustained high-level performance and long-term health.
Part 5: Key considerations to make when designing a hip screening/monitoring program to identify athletes that may be at increased risk for injury.
I strongly advise taking the time to go through each of these articles, at some point. I intentionally broke up this article series into many parts to make the content of each article more easily digestible.
General Overview of Treatments
There may come a time when the athlete is faced with the decision of whether or not to get surgery to relieve pain and/or return to previous levels of athletic performance. King et al. (2015) compared return-to-play rates and times between surgical procedures vs. physical therapy/rehabilitation interventions for treatment of athletic groin pain [1]. Return-to-play rates were comparable for surgical vs. rehabilitative interventions for pubic, abdominal, and adductor-related groin pain [1]. However, rehabilitative intervention outperformed the surgical interventions for return-to-play times for pubic and adductor-related groin pain [1]. For pubic-related groin pain, athletes were able to return-to-play 12.6 weeks faster, on average, with rehabilitation, compared with surgery [1]. Although not statistically significant, there was a clinical difference (greater than a week) between treatments for adductor-related groin pain, with rehabilitative techniques resulting in faster return-to-play, compared with their surgical counterparts [1]. The results from this meta-analysis should be interpreted cautiously, however; the authors note that the quality of research in the area of athletic groin pain is poor and comparison between surgical and rehabilitation treatments are lacking [1]. These findings are complemented by another systematic review which concluded that there is compelling evidence from level 4 (lower-quality) studies which indicate that exercise therapy is a beneficial treatment for groin injury in athletes in terms of symptom remission, return to sport, and recurrence outcomes [2].

The most important aspect of addressing groin-related pathology in athletes is the understanding that these injuries are oftentimes complex, with multiple coexisting causes [3]. Despite my attempt to segregate treatment strategies and outcomes by injury-specific signs and symptoms, most of these injuries are multifactorial and should be addressed on a case-by-case basis. Generally, the following 3-step approach is advised for injury recovery: (1) identify the most prominent deficits via clinical testing, (2) address these deficits as soon as possible, and (3) monitor how addressing these deficits affects the progression of clinical signs and symptoms. Although surgery is oftentimes necessary for full return to pain-free sport participation, this article will largely be focused on the different causes of groin pain, and what research on non-surgical treatment strategies suggests, in each scenario.
Adductor and Pubic-Related Groin Pain
In elite soccer athletes, adductor-related groin pain is considered to be the most frequent diagnosis of groin pain, followed by iliopsoas and inguinal-related groin pain (discussed later), [4, 5]. Although limited high quality evidence exists, current research appears to advise that the nonsurgical (less invasive) option should, most likely, include muscle strengthening activities. There was higher return-to-play success when supervised rehabilitation was performed, focusing on muscle strengthening muscles acting on the pelvis (particularly the adductors), compared to the use of passive physical therapy modalities, in athletes with long-standing groin pain [6]. There’s also evidence that adding shockwave therapy to supervised physical training can accelerate return-to-play, compared with physical training alone [7].
It may not be enough to focus solely on strengthening specific muscle groups, in isolation. A recent clinical trial found remarkable success when individualized rehabilitation programs focusing on intersegmental control and muscular strength were administered [8]. King et al. (2016) administered rehabilitation programs focused on intersegmental control in 205 male, multi-directional athletes with longstanding athletic groin pain [8]. Faster pain-free return-to-play (RTP) rates and times (73% RTP, 9.9±3.4 weeks) were observed, compared with previous anatomically-specific rehabilitation protocols (48-68% RTP, 17.3-18.5 weeks) [6, 9] as well as with surgical protocols for adductor (63%-76%?RTP, 14-18 weeks) [10-12], and pubic pathology (100% RTP, 13–28 weeks) [13, 14].

Another group of researchers observed faster return-to-play when injured athletes performed a multi-modal program including (1) heat, (2) Van den Akker manual therapy, (3) stretching, and (4) a return to running program, compared with unsupervised exercise therapy, combined with the same return to running program [9].
Overall, it appears that using a multi-modal program incorporating a heavy dose of progressive, intersegmental muscle strengthening exercises is a viable strategy for treating most forms of adductor-related groin pain. It goes without saying that the muscles acting on the pelvis (primarily the hip adductors) should be of primary focus [15]. Since the clinical difference between adductor-related and pubic-related pain in the current literature is negligible, it’s advisable to treat both situations similarly [16].
Athletic Pubalgia and Inguinal-Related Groin Pain
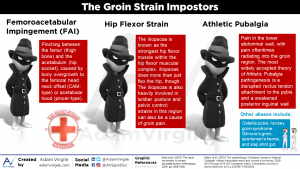
Athletic Pubalgia is a core muscle injury, and is a common cause of chronic groin pain in athletes [17]. The injury is categorized by pain in the lower abdominal wall, with pain, oftentimes, radiating into the groin region [18, 19]. Other terms used to describe Athletic Pubalgia include osteitis pubis, hockey groin syndrome, Gilmore’s groin, sportsman’s hernia, and slap shot gut [18, 19]. Inguinal hernias present themselves in the same area as Athletic Pubalgia (i.e. the lower abdomen). However, an inguinal hernia is specific to the inguinal canal, an area just above of the groin region.
There are cases to be made for both surgical, and nonsurgical treatment options for Athletic Pubalgia. For athletes with chronic groin pain and suspected sportsman’s hernia (i.e. Athletic Pubalgia), surgery resulted in lower pain and a higher percentage of return to play than nonsurgical treatment [20]. Similarly, Meyers et al. (2000) reported marked success with surgical procedures to alleviate Athletic Pubalgia in high-level athletes [21]. Surgical approaches used to treat Athletic Pubalgia have resulted in 80% to 97% chance for return to competitive sport [22, 23]. With proper post-operative rehabilitation, athletes are typically able to make a complete return to sporting activities within 1-2 months [24-26].
In athletes invited to the NFL Combine between 2012-2015, there was little difference in on-field or physical performance at the NFL Combine between players who had hernia surgery, compared with players who did not have surgery [26]. In another study involving NFL players, although there were no significant differences in performance metrics between those who underwent Athletic Pubalgia surgery and matched controls, players who were not operated on ended up playing in more games per season and sustained longer playing careers [22]. In Major League Baseball (MLB) players, inguinal pain is first approached with rest, activity modification, and non-surgical treatment, followed by a rehabilitation program focusing on core strengthening, trunk stabilization, postural training, batting/throwing mechanics, and graduated return to sport protocols [27]. If these means are unsuccessful in returning the athlete to the desired level of activity, surgical treatments are considered [27]. This appears to be the consensus approach for when inguinal-related groin pain presents itself; researchers advise to implement a non-operative approach first, due to the inherent risk of surgical complications [16, 26].

Despite imaging techniques being beyond the scope of this article, Dr. William Meyers gives great overall guidance for practitioners when he states, “the gold standard for precise diagnosis and treatment remains with experienced clinical judgment after digestion of all the clinical and radiologic findings,” [28]. In any case, routinely monitoring hip adductor, hip abductor, and abdominal muscle strength in and around the competitive season is advised because of the relationship between weaknesses in these areas and inguinal-related groin pain [16, 29].
Iliopsoas-Related Groin Pain
The iliopsoas is the strongest hip flexor muscular complex [30] and is comprised of the psoas major, psoas minor, and iliacus muscles [31]. Although considered the primary hip flexor complex, the iliopsoas is also heavily involved in lumbar posture and pelvic control; strains in this region can also contribute to groin pain experienced by athletes [18, 32, 33].
Iliopsoas-related groin pain can be classified as groin pain with resisted hip flexion and/or hip flexor stretching [34, 35]. Based on physical examination, it has been reported that the iliopsoas was the primary cause of groin pain in 17% to 35% of the athletes investigated [36, 37]. Although not always the primary clinical entity, iliopsoas-related pain may contribute to the overall groin pain symptoms [36]. Treatment of iliopsoas-related groin pain should focus on iliopsoas impairments and functional deficits. Surgical repair via arthroscopic iliopsoas release, or tenotomy, has resulted in iliopsoas muscular atrophy and reduced hip flexion strength [38]. As such, surgery is not recommended as first-line treatment [16].
Iliopsoas-related groin pain and hip-related groin pain (discussed in the next section) can occur in unison [39]. It’s not uncommon for an athlete’s groin pain to have more than one cause; 27% to 50% of athletes have presented with multiple clinical causes for their groin pain [3, 34-37]. It’s important to identify and understand the mechanism of injury, and subsequently attempt to address any hip flexion strength deficits, when an athlete presents with iliopsoas-related groin pain [16, 39]. Additionally, given the integral role of the iliopsoas in lumbar posture and pelvic control, strengthening the abdominal musculature is advised for both prevention, and treatment.
Femoroacetabular Impingement (FAI) and Hip-Related Groin Pain
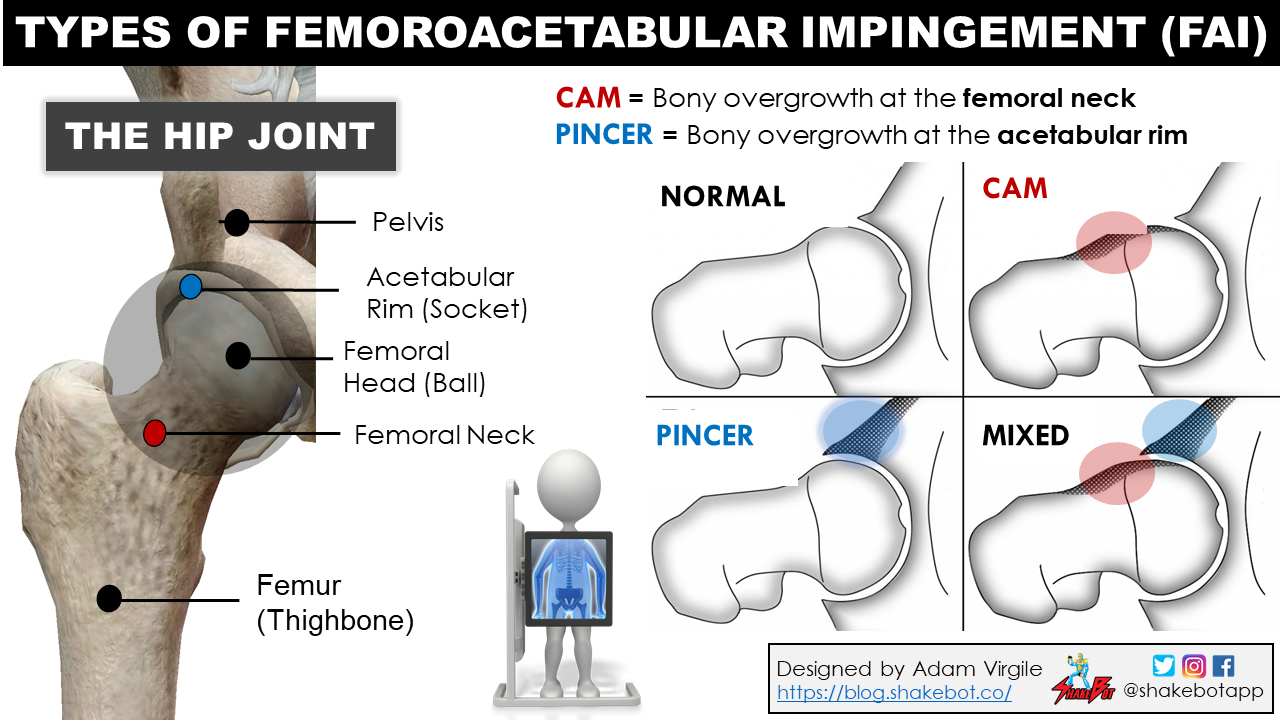
Femoroacetabular impingement (FAI) is the most commonly diagnosed cause of hip-related groin pain in ice hockey players at all ages and levels of play [40-42]. FAI has become an increasingly common diagnosis in ice hockey players but is difficult to differentiate from hip strains because its pathophysiology is poorly understood [43]. FAI refers to pinching between the femur (thigh bone) and the acetabulum (hip socket). This is often caused by bony overgrowth to the femoral neck (CAM-type) or acetabular rim (pincer-type), but the body responds to FAI with inflammation and tightening of the hip capsule, causing compensatory strain to muscles around the hip. FAI is generally associated with hip pain and functional impairments such as limited ROM [44-47], hip muscle weakness [48-50], and compromised athletic performance [42, 50].

Management and treatment strategies for hip-related groin pain (specifically FAI) center around rehabilitation through physical exercises, medication, and surgery (most notably arthroscopy), [51]. Current evidence doesn’t support the superiority of any single management strategy, at this time. Hip-related groin pain (i.e. FAI) is typically associated with hip muscle weakness [52-54], particularly in the hip flexors and adductors [45, 48]. Additionally, the most common intra-articular hip injury in NHL players, the labral tear [55], is often the result of underlying FAI.
Bonus Section: A Short Rant on Early Ice Hockey Specialization and FAI Risk
Single sport specialization can be defined as intensive year-round training in one sport to the exclusion of others [56]. Many young athletes, parents, and coaches believe that early single-sport specialization is necessary for long-term athletic success [57-61]. These perceptions are short-sighted, potentially detrimental to the athlete’s short-term and long-term health, and oftentimes are conceived on unrealistic expectations.
Even if athletic success is attained at the youth level, research supporting its translation into long-term senior success is iffy, at best [62-66]. In other words, early competitive athletic success is not a prerequisite, nor a valid predictor of long-term athletic accomplishment. In fact, a recent review highlighted that the youth participation patterns that lead to youth success are quite different than those that facilitate long-term athletic development and adult success [67].
I’ll present an in-depth take on single sport specialization vs. sport diversity during youth in a separate post on long-term athletic development, but right now, let’s briefly focus on early sport specialization and how it may impact injury risk.
Early specialization in a single sport appears to be a decent strategy for attaining youth athletic success. There are many reports suggesting that early single sport specialization and intensified, sport-specific practice/training during childhood (age ??12 years) and adolescence (13–18 years) correlate with youth athletic success [68-74]. On the surface, it appears that early sport specialization is the ideal path for climbing up the ranks, and eventually reaching sport performance at the highest level possible.
In 2008, Malcolm Gladwell authored his book, Outliers, popularizing the “10,000 hour rule,” [75]. Through studying the most successful business professionals and musicians throughout history and their paths to success, Gladwell discovered the true mastery of a skill requires 10,000 hours of deliberate practice [75]. Many believe that 10,000 hours of deliberate practice are necessary for sport mastery, as well [76].
Many athletes and coaches report that it would be foolish to not specialize in a single sport early on because increased recognition, attainment of professional status, a college scholarship, or an Olympic qualification could result [77]. One of the world’s most renowned athletes, Tiger Woods, is a prime example supporting the advocates of early sport specialization [78]. At a mere 12 years of age, Tiger recorded his first round of 70 on a regulation golf course. At age 20 in 1996, Tiger became the first golfer to win three consecutive U.S. Amateur titles and won the NCAA individual golf championship [78]. Tiger’s early introduction to golf, deliberate practice at a very early age, a dominating parent in Earl Woods, a highly regulated life through childhood and adolescence into adulthood, and eventual extraordinary athletic success is a well-documented story [79]. Tiger undoubtedly accrued 10,000 hours of deliberate practice early in his career and achieved sport mastery, as advised by Malcolm Gladwell.
Given this mindset, it’s no surprise that early sport specialization is becoming more prevalent as time goes on [80-84]. Specific to ice hockey, a recent study in Ontario Hockey League (OHL) players found an increased commitment to hockey at a younger age, compared with older studies [85]. At 14 years old, most players had abandoned playing other sports, and had decided to try to become elite athletes, and spent virtually all of their available time training for hockey, thereby showing that they had invested in hockey [85]. Similarly, a recent report by the NCAA revealed that 59% of collegiate male ice hockey athletes specialize in their sport by the age of 12 [86].
So, what does any of this early sport specialization business have to do with femoroacetabular impingement (FAI), you ask?
Growth spurts typical occur between the ages 10-16 in males. In the previous section, we learned that hockey players likely become specialized during this time as they have abandoned all other sports before they reach 14 years of age. There’s an elevated risk for injury during the adolescent growth spurt [87], particularly involving the apophysis and physis (i.e. the ends) of bones [88-90], when repetitive activity is performed. For example, the increasing rate of ulnar collateral ligament injuries in baseball pitchers and traumatic knee injuries (i.e. ACL tears) in younger athletes is oftentimes attributed to increasing rates of early single sport specialization and resulting overuse [91-95]. Similarly, early specialization in ice hockey and the resulting repetitive stresses through the hip could affect physis and apophysis alterations in the femur.
Philippon et al. (2013) performed a study of 61 asymptomatic youth hockey players (10-18 years old) where the alpha angle was assessed in multiple age groups and compared with skiers as a control population [96]. The ice hockey players had a higher alpha angle associated with CAM-type impingement (overgrowth of the femoral neck) and, importantly, this incidence increased with age and athletic participation [96]. Alpha angle, which measures the extent to which the femoral head deviates from spherical [97], is commonly used to assess the presence of CAM-type impingement [98]. Although the individual number of hours training was not quantified, this is one of the few studies demonstrating that sport specialization in youth athletics can lead to detrimental bony changes during growth. The authors concluded that high levels of participation in ice hockey can increase the risk for the development of CAM-type hip impingement and hip labral tears [96].

A similar study performed in Switzerland evaluated 77 elite hockey players with a questionnaire, clinical examination, and imaging. At a mere 16.5 years of age (on average), 20% of these elite hockey players had a history of hip pain and a positive impingement test finding [99]. The alpha angles were higher in athletes with closed physes versus open physes, and symptomatic athletes had higher alpha angles and reduced internal hip range of motion, compared with asymptomatic athletes. Thus, the authors concluded that FAI may represent an overuse injury from playing ice hockey at an elite level during childhood [99].
Risk factors for FAI include on-ice exposure and younger start ages and the prevalence of FAI increases with age, indicating that hockey-specific movements may lead to increased likelihood for FAI development. A recent review investigating high-level youth sport participation and FAI risk concluded that excessive activity during the adolescent growth period may play a key role in the development of FAI [100]. Particularly, males who participate in ice-hockey, basketball and to a lesser extent soccer, whilst performing a minimum of three training sessions and games per week, are proposed to be at greatest risk for FAI (CAM-deformity) and potentially progressing to symptomatic hip impingement [100]. Overall, FAI, and other hip-related pathologies are oftentimes multifaceted and complex. However, given the aforementioned research, it’s my evidence-based opinion that avoiding a drastic imbalance between on-ice activity and participation in other physical activities (i.e. free play, other sports, resistance training) during youth may help to reduce risk for FAI, among other hip ailments in young hockey players.
From this post, you may have gotten a sense that early sport specialization is a good idea. In 99% of cases, it’s not (in my humble opinion). In a later post, I will provide a general overview of the benefits and drawbacks of early sport specialization, and propose strategies for optimal long-term athletic development.
UPDATE: My article series on early sport specialization begins here.
Part 1: A review of the research investigating the true odds of becoming a collegiate or professional athlete.
Part 2: Whether or not early sport specialization leads to long-term athletic success.
Part 3: How early sport specialization increases injury risk and can lead to athlete burnout.
Part 4: 5 simple strategies to help prevent athlete burnout.
Part 5: Sport volume recommendations for youth athletes.
Part 6: How organized youth sport impacts family dynamics.
Reference:
- King, E., Ward, J., Small, L., Falvey, E. and Franklyn-Miller, A., 2015. Athletic groin pain: a systematic review and meta-analysis of surgical versus physical therapy rehabilitation outcomes. Br J Sports Med?, ?49?(22), pp.1447-1451.
- Charlton, P.C., Drew, M.K., Mentiplay, B.F., Grimaldi, A. and Clark, R.A., 2017. Exercise interventions for the prevention and treatment of groin pain and injury in athletes: a critical and systematic review. ?Sports Medicine?, ?47?(10), pp.2011-2026.
- Weir, A., 2017. Multidisciplinary Assessment of 100 Athletes With Groin Pain Using the Doha Agreement: High Prevalence of Adductor-Related Groin Pain in Conjunction With Multiple Causes.
- Werner, J., Hägglund, M., Waldén, M. and Ekstrand, J., 2009. UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. British journal of sports medicine, 43(13), pp.1036-1040.
- Hölmich, P., Thorborg, K., Dehlendorff, C., Krogsgaard, K. and Gluud, C., 2013. Incidence and clinical presentation of groin injuries in sub-elite male soccer. Br J Sports Med, pp.bjsports-2013.
- Hölmich, P., Uhrskou, P., Ulnits, L., Kanstrup, I.L., Nielsen, M.B., Bjerg, A.M. and Krogsgaard, K., 1999. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. ?The Lancet?, ?353?(9151), pp.439-443.
- Schöberl, M., Prantl, L., Loose, O., Zellner, J., Angele, P., Zeman, F., Spreitzer, M., Nerlich, M. and Krutsch, W., 2017. Non-surgical treatment of pubic overload and groin pain in amateur football players: a prospective double-blinded randomised controlled study. ?Knee Surgery, Sports Traumatology, Arthroscopy?, ?25?(6), pp.1958-1966.
- King, E., Franklyn-Miller, A., Richter, C., O’Reilly, E., Doolan, M., Moran, K., Strike, S. and Falvey, É., 2018. Clinical and biomechanical outcomes of rehabilitation targeting intersegmental control in athletic groin pain: prospective cohort of 205 patients. ?Br J Sports Med?, pp.bjsports-2016.
- Weir A, Jansen JA, van de Port IG, Van de Sande HB, Tol JL, Backx FJ. Manual or exercise therapy for long-standing adductor-related groin pain: a randomised controlled clinical trial. Man Ther. 2011; 16: 148– 150
- Akermark, C. and Johansson, C., 1992. Tenotomy of the adductor longus tendon in the treatment of chronic groin pain in athletes. The American journal of sports medicine, 20(6), pp.640-643.
- Maffulli, N., Loppini, M., Longo, U.G. and Denaro, V., 2012. Bilateral mini-invasive adductor tenotomy for the management of chronic unilateral adductor longus tendinopathy in athletes. The American journal of sports medicine, 40(8), pp.1880-1886.
- Robertson, I.J., Curran, C., McCaffrey, N., Shields, C.J. and McEntee, G.P., 2011. Adductor tenotomy in the management of groin pain in athletes. International journal of sports medicine, 32(01), pp.45-48.
- Hechtman, K.S., Zvijac, J.E., Popkin, C.A., Zych, G.A. and Bemden, A.B.V., 2010. A minimally disruptive surgical technique for the treatment of osteitis pubis in athletes. Sports Health, 2(3), pp.211-215.
- Williams, P.R., Thomas, D.P. and Downes, E.M., 2000. Osteitis pubis and instability of the pubic symphysis: when nonoperative measures fail. The American journal of sports medicine, 28(3), pp.350-355.
- Tyler, T.F., Silvers, H.J., Gerhardt, M.B. and Nicholas, S.J., 2010. Groin injuries in sports medicine. ?Sports health?, ?2?(3), pp.231-236.
- Thorborg, K., Reiman, M.P., Weir, A., Kemp, J.L., Serner, A., Mosler, A.B. and Hölmich, P., 2018. Clinical examination, diagnostic imaging, and testing of athletes with groin pain: an evidence-based approach to effective management. journal of orthopaedic & sports physical therapy, 48(4), pp.239-249.
- Arner, J.W., Disantis, A., Bradley, J.P., Zuckerbraun, B.S. and Mauro, C.S., 2017. Management of hip and groin pain in American football players. Annals of Joint, 2(12).
- Kuhn, A.W., Noonan, B.C., Kelly, B.T., Larson, C.M. and Bedi, A., 2016. The hip in ice hockey: A current concepts review. Arthroscopy, 32(9), pp.1928-1938.
- Serner, A., van Eijck, C.H., Beumer, B.R., Hölmich, P., Weir, A. and de Vos, R.J., 2015. Study quality on groin injury management remains low: a systematic review on treatment of groin pain in athletes. ?Br J Sports Med?, pp.bjsports-2014.
- Paajanen H, Brinck T, Hermunen H, Airo I. Laparoscopic surgery for chronic groin pain in athletes is more effective than nonoperative treatment: a randomized clinical trial with magnetic resonance imaging of 60 patients with sportsman’s hernia (athletic pubalgia). Surgery. 2011; 150: 99– 107.
- Meyers, W.C., Foley, D.P., Garrett, W.E., Lohnes, J.H. and Mandlebaum, B.R., 2000. Management of severe lower abdominal or inguinal pain in high-performance athletes. ?The American journal of sports medicine?, ?28?(1), pp.2-8.
- Jack, R.A., Evans, D.C., Echo, A., McCulloch, P.C., Lintner, D.M., Varner, K.E. and Harris, J.D., 2017. Performance and return to sport after sports hernia surgery in NFL players. Orthopaedic Journal of Sports Medicine, 5(4), p.2325967117699590.
- Larson, C.M., 2014. Sports hernia/athletic pubalgia: evaluation and management. Sports Health, 6(2), pp.139-144.
- Susmallian, S., Ezri, T., Elis, M., Warters, R., Charuzi, I. and Muggia-Sullam, M., 2004. Laparoscopic repair of ‘sportsman’s hernia’in soccer players as treatment of chronic inguinal pain. Medical Science Monitor, 10(2), pp.CR52-CR54.
- Kluin, J., den Hoed, P.T., van Linschoten, R., Ijzerman, J.C. and van Steensel, C.J., 2004. Endoscopic evaluation and treatment of groin pain in the athlete. The American journal of sports medicine, 32(4), pp.944-949.
- Knapik, D.M., Gebhart, J.J., Nho, S.J., Tanenbaum, J.E., Voos, J.E. and Salata, M.J., 2017. Prevalence of surgical repair for athletic pubalgia and impact on performance in football athletes participating in the National Football League Combine. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 33(5), pp.1044-1049.
- Mlynarek, R.A. and Coleman, S.H., 2018. Hip and Groin Injuries in Baseball Players. Current reviews in musculoskeletal medicine, 11(1), pp.19-25.
- Meyers, W.C., 2017. Editorial Commentary: Core Muscle Injuries or Athletic Pubalgia—Finally the Real Sausage, Not Just the Same Ole Baloney.
- Hölmich, P., Uhrskou, P., Ulnits, L., Kanstrup, I.L., Nielsen, M.B., Bjerg, A.M. and Krogsgaard, K., 1999. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. ?The Lancet?, ?353?(9151), pp.439-443.
- Robbins, C.E., 1998. Anatomy and biomechanics. The Hip Handbook. Boston, MA: Butterworth-Heinemann, pp.1-37.
- Hughes, P.E., Hsu, J.C. and Matava, M.J., 2002. Hip anatomy and biomechanics in the athlete. Sports medicine and arthroscopy review, 10(2), pp.103-114.
- Emery, C.A., Meeuwisse, W.H. and Powell, J.W., 1999. Groin and abdominal strain injuries in the National Hockey League. ?Clinical journal of sport medicine: official journal of the Canadian Academy of Sport Medicine?, ?9?(3), pp.151-156.
- Andersson, E., Oddsson, L., Grundström, H. and Thorstensson, A., 1995. The role of the psoas and iliacus muscles for stability and movement of the lumbar spine, pelvis and hip. Scandinavian journal of medicine & science in sports?, ?5?(1), pp.10-16.
- Weir, A., Brukner, P., Delahunt, E., Ekstrand, J., Griffin, D., Khan, K.M., Lovell, G., Meyers, W.C., Muschaweck, U., Orchard, J. and Paajanen, H., 2015. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br J Sports Med, 49(12), pp.768-774.
- Rankin, A.T., Bleakley, C.M. and Cullen, M., 2015. Hip joint pathology as a leading cause of groin pain in the sporting population: a 6-year review of 894 cases. ?The American journal of sports medicine?, ?43?(7), pp.1698-1703.
- Hölmich, P., 2007. Long-standing groin pain in sportspeople falls into three primary patterns, a “clinical entity” approach: a prospective study of 207 patients. ?British journal of sports medicine?, ?41?(4), pp.247-252.
- Serner, A., Tol, J.L., Jomaah, N., Weir, A., Whiteley, R., Thorborg, K., Robinson, M. and Hölmich, P., 2015. Diagnosis of acute groin injuries: a prospective study of 110 athletes. ?The American journal of sports medicine?, ?43?(8), pp.1857-1864.
- Brandenburg, J.B., Kapron, A.L., Wylie, J.D., Wilkinson, B.G., Maak, T.G., Gonzalez, C.D. and Aoki, S.K., 2016. The functional and structural outcomes of arthroscopic iliopsoas release. ?The American journal of sports medicine?, ?44?(5), pp.1286-1291.
- Serner, A., 2017. Diagnosis of acute groin injuries in athletes. Br J Sports Med, pp.bjsports-2017.
- Stull, J.D., Philippon, M.J. and LaPrade, R.F., 2011. “At-risk” positioning and hip biomechanics of the Peewee ice hockey sprint start. The American journal of sports medicine, 39(1_suppl), pp.29-35.
- Ayeni, O.R., Kowalczuk, M., Farag, J., Farrokhyar, F., Chu, R., Bedi, A., Willits, K. and Bhandari, M., 2014. Trends in reporting of mechanisms and incidence of hip injuries in males playing minor ice hockey in Canada: a cross-sectional study. Open access journal of sports medicine, 5, p.143.
- Shindle, M.K., Marx, R.G., Kelly, B.T., Bisson, L. and Burke III, C.J., 2010. Hockey injuries: a pediatric sport update. ?Current opinion in pediatrics?, ?22?(1), pp.54-60.
- Dalton, S.L., Zupon, A.B., Gardner, E.C., Djoko, A., Dompier, T.P. and Kerr, Z.Y., 2016. The epidemiology of hip/groin injuries in national collegiate athletic association men’s and women’s ice hockey: 2009-2010 through 2014-2015 academic years. Orthopaedic journal of sports medicine, 4(3), p.2325967116632692.
- Nötzli, H.P., Wyss, T.F., Stoecklin, C.H., Schmid, M.R., Treiber, K. and Hodler, J., 2002. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. ?Bone & Joint Journal?, ?84?(4), pp.556-560.
- Casartelli, N.C., Maffiuletti, N.A., Leunig, M. and Bizzini, M., 2015. Femoroacetabular impingement in sports medicine: a narrative review. ?Schweizerische Zeitschrift für Sportmedizin & Sporttraumatologie?, 63?(2).
- ?Yuan, B.J., Bartelt, R.B., Levy, B.A., Bond, J.R., Trousdale, R.T. and Sierra, R.J., 2013. Decreased range of motion is associated with structural hip deformity in asymptomatic adolescent athletes. ?The American journal of sports medicine?, ?41?(7), pp.1519-1525.
- Lerebours, F., Robertson, W., Neri, B., Schulz, B., Youm, T. and Limpisvasti, O., 2016. Prevalence of cam-type morphology in elite ice hockey players. ?The American journal of sports medicine?, ?44?(4), pp.1024-1030.
- Casartelli, N.C., Maffiuletti, N.A., Item-Glatthorn, J.F., Staehli, S., Bizzini, M., Impellizzeri, F.M. and Leunig, M., 2011. Hip muscle weakness in patients with symptomatic femoroacetabular impingement. Osteoarthritis and cartilage?, ?19?(7), pp.816-821.
- ?Brunner, R., Maffiuletti, N.A., Casartelli, N.C., Bizzini, M., Sutter, R., Pfirrmann, C.W. and Leunig, M., 2016. Prevalence and functional consequences of femoroacetabular impingement in young male ice hockey players. ?The American journal of sports medicine?, ?44?(1), pp.46-53.
- ?Casartelli, N.C., Leunig, M., Maffiuletti, N.A. and Bizzini, M., 2015. Return to sport after hip surgery for femoroacetabular impingement: a systematic review. ?Br J Sports Med?, pp.bjsports-2014.
- Griffin, D.R., Dickenson, E.J., O’donnell, J., Awan, T., Beck, M., Clohisy, J.C., Dijkstra, H.P., Falvey, E., Gimpel, M., Hinman, R.S. and Hölmich, P., 2016. The Warwick Agreement on femoroacetabular impingement syndrome (FAI syndrome): an international consensus statement. ?Br J Sports Med?, ?50?(19), pp.1169-1176.
- Nepple, J.J., Goljan, P., Briggs, K.K., Garvey, S.E., Ryan, M. and Philippon, M.J., 2015. Hip strength deficits in patients with symptomatic femoroacetabular impingement and labral tears.Arthroscopy,? 31?(11),? pp.2106-2111.
- ?Freke, M.D., Kemp, J., Svege, I., Risberg, M.A., Semciw, A. and Crossley, K.M., 2016. Physical impairments in symptomatic femoroacetabular impingement: a systematic review of the evidence. ?Br J Sports Med?, pp.bjsports-2016.
- Mayne, E., Memarzadeh, A., Raut, P., Arora, A. and Khanduja, V., 2017. Measuring hip muscle strength in patients with femoroacetabular impingement and other hip pathologies: A systematic review. ?Bone and Joint Research?, ?6?(1), pp.66-72.
- Gallo, R.A., Silvis, M.L., Smetana, B., Stuck, D., Lynch, S.A., Mosher, T.J. and Black, K.P., 2014. Asymptomatic hip/groin pathology identified on magnetic resonance imaging of professional hockey players: Outcomes and playing status at 4 years’ follow-up. ?Arthroscopy?, ?30?(10), pp.1222-1228.
- Myer, G.D., Jayanthi, N., Difiori, J.P., Faigenbaum, A.D., Kiefer, A.W., Logerstedt, D. and Micheli, L.J., 2015. Sport specialization, part I: does early sports specialization increase negative outcomes and reduce the opportunity for success in young athletes?. Sports Health, 7(5), pp.437-442.
- Brooks, M.A., Post, E.G., Trigsted, S.M., Schaefer, D.A., Wichman, D.M., Watson, A.M., McGuine, T.A. and Bell, D.R., 2018. Knowledge, Attitudes, and Beliefs of Youth Club Athletes Toward Sport Specialization and Sport Participation. Orthopaedic journal of sports medicine, 6(5), p.2325967118769836.
- Voigt, L. and Hohmann, A., 2016. Expert youth coaches’ diversification strategies in talent development: A qualitative typology. International Journal of Sports Science & Coaching, 11(1), pp.39-53.
- Malina, R.M., 2010. Early sport specialization: roots, effectiveness, risks. Current sports medicine reports, 9(6), pp.364-371.
- Padaki, A.S., Ahmad, C.S., Hodgins, J.L., Kovacevic, D., Lynch, T.S. and Popkin, C.A., 2017. Quantifying Parental Influence on Youth Athlete Specialization: A Survey of Athletes’ Parents. Orthopaedic journal of sports medicine, 5(9), p.2325967117729147.
- Padaki, A.S., Popkin, C.A., Hodgins, J.L., Kovacevic, D., Lynch, T.S. and Ahmad, C.S., 2017. Factors that drive youth specialization. Sports health, 9(6), pp.532-536.
- Brouwers, J., De Bosscher, V. and Sotiriadou, P., 2012. An examination of the importance of performances in youth and junior competition as an indicator of later success in tennis. Sport Management Review, 15(4), pp.461-475.
- Schumacher, Y.O., Mroz, R., Mueller, P., Schmid, A. and Ruecker, G., 2006. Success in elite cycling: A prospective and retrospective analysis of race results. Journal of Sports Sciences, 24(11), pp.1149-1156.
- Barreiros, A., Côté, J. and Fonseca, A.M., 2014. From early to adult sport success: Analysing athletes’ progression in national squads. European Journal of Sport Science, 14(sup1), pp.S178-S182.
- Güllich, A. and Emrich, E., 2014. Considering long-term sustainability in the development of world class success. European Journal of Sport Science, 14(sup1), pp.S383-S397.
- Vaeyens, R., Güllich, A., Warr, C.R. and Philippaerts, R., 2009. Talent identification and promotion programmes of Olympic athletes. Journal of sports sciences, 27(13), pp.1367-1380.
- Araújo, D., Shuttleworth, R., Güllich, A. and Davids, K., 2017. Understanding environmental and task constraints on talent development: Analysis of micro-structure of practice and macro-structure of development histories. In Routledge Handbook of Talent Identification and Development in Sport(pp. 220-234). Routledge.
- Cathey, R.M., 2010. Retrospective practice histories of expert and novice baseball pitchers (Doctoral dissertation, University of South Carolina).
- Ford, P.R., Ward, P., Hodges, N.J. and Williams, A.M., 2009. The role of deliberate practice and play in career progression in sport: the early engagement hypothesis. High ability studies, 20(1), pp.65-75.
- Elferink-Gemser, M.T., Visscher, C., Lemmink, K.A. and Mulder, T., 2007. Multidimensional performance characteristics and standard of performance in talented youth field hockey players: A longitudinal study. Journal of sports sciences, 25(4), pp.481-489.
- Ford, P.R. and Williams, A.M., 2012. The developmental activities engaged in by elite youth soccer players who progressed to professional status compared to those who did not. Psychology of sport and exercise, 13(3), pp.349-352.
- Haugaasen, M. and Jordet, G., 2012. Developing football expertise: a football-specific research review. International Review of Sport and Exercise Psychology, 5(2), pp.177-201.
- Ward, P., Hodges, N.J., Williams, A.M. and Starkes, J.L., 2004. 11 Deliberate practice and expert performance. Skill acquisition in sport: Research, theory and practice, p.231.
- Weissensteiner, J., Abernethy, B., Farrow, D. and Müller, S., 2008. The development of anticipation: A cross-sectional examination of the practice experiences contributing to skill in cricket batting. Journal of Sport and Exercise Psychology, 30(6), pp.663-684.
- Gladwell M. Outliers: The Story of Success. New York, NY: Little, Brown and Company; 2008.
- Starkes, J.L. and Ericsson, K.A., 2003. Expert performance in sports: Advances in research on sport expertise. Human Kinetics.
- Wiersma, L.D., 2000. Risks and benefits of youth sport specialization: Perspectives and recommendations. Pediatric Exercise Science, 12(1), pp.13-22.
- TOGETHER, WE CAN MAKE THE FUTURE SHINE BRIGHT!” Tiger Woods, tigerwoods.com/biography/
- Farrey T. Game On: The All-American Race to Make Champions of Our Children. New York: ESPN Books, 2008.
- Jayanthi, N.A., LaBella, C.R., Fischer, D., Pasulka, J. and Dugas, L.R., 2015. Sports-specialized intensive training and the risk of injury in young athletes: a clinical case-control study. The American journal of sports medicine, 43(4), pp.794-801.
- Buckley, P.S., Bishop, M., Kane, P., Ciccotti, M.C., Selverian, S., Exume, D., Emper, W., Freedman, K.B., Hammoud, S., Cohen, S.B. and Ciccotti, M.G., 2017. Early Single-Sport Specialization: A Survey of 3090 High School, Collegiate, and Professional Athletes. Orthopaedic journal of sports medicine, 5(7), p.2325967117703944.
- Hill, G.M. and Simons, J., 1989. A study of the sport specialization on high school athletics. Journal of Sport and Social Issues, 13(1), pp.1-13.
- Metzl, J.D., 2002. Expectations of pediatric sport participation among pediatricians, patients, and parents. Pediatric Clinics of North America, 49(3), pp.497-504.
- Bell, D.R., Post, E.G., Trigsted, S.M., Hetzel, S., McGuine, T.A. and Brooks, M.A., 2016. Prevalence of sport specialization in high school athletics: a 1-year observational study. The American journal of sports medicine, 44(6), pp.1469-1474.
- Garland, W.J., 2017. Developmental Activities of Ontario Hockey League Players.
- Schwarb, A. W. (2016, April 19). After school specialized: Studies discourage specialization for young athletes. NCAA Champion Magazine, Spring. Retrieved from http://www.ncaa.org/champion/after-school-specialized
- Caine, D., Cochrane, B., Caine, C. and Zemper, E., 1989. An epidemiologic investigation of injuries affecting young competitive female gymnasts. The American journal of sports medicine, 17(6), pp.811-820.
- Caine, D., DiFiori, J. and Maffulli, N., 2006. Physeal injuries in children’s and youth sports: reasons for concern?. British journal of sports medicine, 40(9), pp.749-760.
- DiFiori, J.P., 2010. Evaluation of overuse injuries in children and adolescents. Current sports medicine reports, 9(6), pp.372-378.
- DiFiori, J.P., 2010. Overuse injury of the physis: a “growing” problem.
- American Sports Medicine Institute. Position statement for youth baseball pitchers. 2013. Available at: http://www.asmi.org/research.php?page5research §ion5positionStatement. Accessed October 17, 2014.
- Petty DH, Andrews JR, Fleisig GS, et al. Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med 2004;32:1158–64.
- Savoie FH 3rd, Trenhaile SW, Roberts J, et al. Primary repair of ulnar collateral ligament injuries of the elbow in young athletes: a case series of injuries to the proximal and distal ends of the ligament. Am J Sports Med 2008;36:1066–72.
- Zell M, Dwek JR, Edmonds EW. Origin of the medial ulnar collateral ligament on the pediatric elbow. J Child Orthop 2013;7:323–8.
- Larsen N, Moisan A, Witte D, et al. Medial ulnar collateral ligament origin in children and adolescents: an MRI anatomic study. J Pediatr Orthop 2013;33:664–6
- Philippon, M.J., Ho, C.P., Briggs, K.K., Stull, J. and LaPrade, R.F., 2013. Prevalence of increased alpha angles as a measure of cam-type femoroacetabular impingement in youth ice hockey players. The American journal of sports medicine, 41(6), pp.1357-1362.
- Nötzli, H.P., Wyss, T.F., Stoecklin, C.H., Schmid, M.R., Treiber, K. and Hodler, J., 2002. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. The Journal of bone and joint surgery. British volume, 84(4), pp.556-560.
- Waarsing, J.H., Thomas, G.E., Carr, A.J., Reijman, M., Bierma-Zeinstra, S.M.A., Glyn-Jones, S., Weinans, H. and Arden, N.K., 2014. Cam impingement: defining the presence of a cam deformity by the alpha angle: data from the CHECK cohort and Chingford cohort. Osteoarthritis and cartilage, 22(2), pp.218-225.
- Siebenrock, K.A., Kaschka, I., Frauchiger, L., Werlen, S. and Schwab, J.M., 2013. Prevalence of cam-type deformity and hip pain in elite ice hockey players before and after the end of growth. The American journal of sports medicine, 41(10), pp.2308-2313.
- Zadpoor, A.A., 2015. Etiology of femoroacetabular impingement in athletes: a review of recent findings. Sports Medicine, 45(8), pp.1097-1106.