Monitoring body composition in athletes is beneficial for a myriad of reasons. DXA, or dual-energy X-ray absorptometry, is one of many methods that can be used to assess body composition in athletes. How DXA works, its popularity, and sources and margin of error are reviewed in this article.
How DXA Works
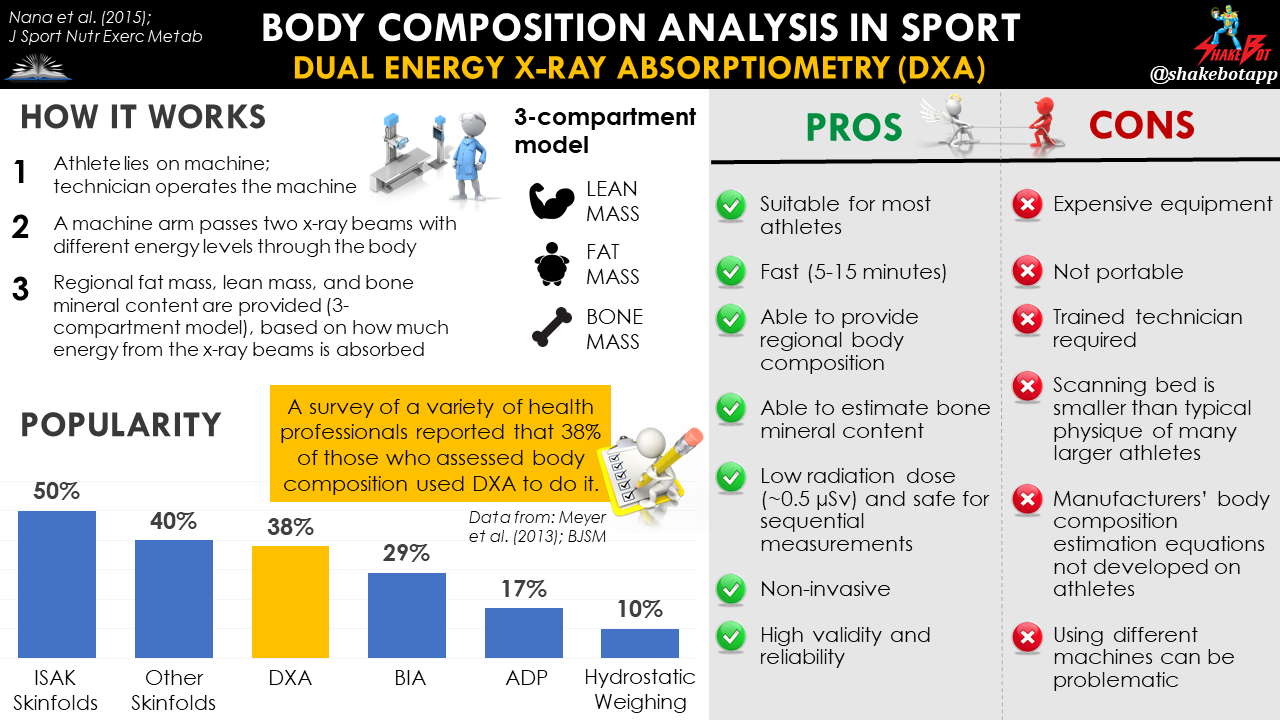
Dual-energy X-ray absorptiometry (DXA) uses attenuation of calibrated X-ray beams with dual photon energy (emitting a very small dose of ionizing radiation) to produce pictures of the inside of the body. The DXA machine sends these thin, low-dose x-rays with two distinct energy peaks through the body. One peak is absorbed mainly by soft tissue and the other by bone. Therefore, DXA is a three-compartment model of body composition as it segregates the body into 3 compartments: fat mass, lean mass, and bone [1]. The fact that DXA can quantify regional bone mass (and bone density) is what sets DXA apart from the remainder of the body composition methods.
Popularity
DXA is the most widely utilized technique for measuring body composition [2], and is considered the “gold standard” body composition measurement tool for athletes [3-7]. In a 2013 survey, 60% and 40% of international and national sport professionals, respectively, were found to use DXA for measuring body composition [8]. DXA is frequently used as the reference measure to assess the validity of other body composition assessment protocols [9-15].

Nana et al. (2015). Methodology review: using dual-energy X-ray absorptiometry (DXA) for the assessment of body composition in athletes and active people. International Journal of Sport Nutrition and Exercise Metabolism, 25(2), pp.198-215.
Biological Error Considerations
It must be noted that the validity of DXA is reduced in very lean, or highly obese subjects, as several researchers have shown underestimation and overestimation of fat mass in very lean and obese individuals, respectively [16]. There are a few key biological (day-to-day) aspects of assessment that can affect measurement variability, or error. Biological variation, including differences in food [17] or fluid [18] intake, and previous exercise [19, 20] can influence DXA results. Alteration of intramuscular solutes (i.e. glycogen, creatine, carnosine), and their associated water-binding properties is another source of biological variation [21-23]. To avoid misinterpretation of the data, it’s essential to understand the biological context of the athlete during data collection, and, if possible, ensure the context remains consistent for the squad of athletes, as well as for each athlete, longitudinally.
For example, an athlete that commences creatine supplementation, or embarks on a higher-carbohydrate diet may have artificially elevated lean mass via DXA, whereas an athlete that embarks on a lower-carbohydrate diet or abstains from creatine supplementation, may have artificially lower lean mass values [21]. If measurements are taken the day following a game or match, athletes who participated in the event may have artificially lower lean mass values due to decrements in muscle glycogen stores, and/or dehydration, compared with athletes that did not participate in such high volumes of high-intensity activity [21, 24]. Although oftentimes uncontrollable, it’s important to understand the impact that these biological contextual factors can have on the DXA results, at the very least.
Technical Error Considerations
Additionally, there are a few key technical (machine/technician) aspects that can affect measurement validity (accuracy) and reliability (consistency). Prone vs. supine subject positioning [25, 26], and even inconsistent clothing worn during assessment [20] can impact results. Using different DXA machine manufacturers [27-29] or scan speeds [30], changing software platforms [31, 32], or altering beam technology within the same manufacturer’s product [33, 34] are not advised because these factors can also influence results.
The different technologies used to scan the body amongst DXA devices include pencil and fan beam technologies. These different technologies, or beams, are pretty easy to comprehend; pencil beam technology uses narrow x-ray beams (i.e. like a pencil), whereas fan beam technology uses wider x-ray beams (i.e. spread out, like a fan). Although fan beams allow faster scanning and better image resolution, these benefits come at a slightly higher cost of radiation exposure [35]. As stated earlier, it’s important to understand the beam technology being used and remain consistent with the beam type to ensure that longitudinal results are reliable.
| Biological Sources of Error | Technical Sources of Error |
| Inconsistent food and fluid intake | Changing DXA machine manufacturer or changs in product specs |
| Inconsistent previous exercise | Inconsistent scanning speed |
| Supplementation that may impact intramuscular solutes with water-binding properties (i.e. creatine, carnosine, glycogen) | Altering beam technology, even within same manufacturer’s product |
| Changes in body size (may overestimate fat mass in very large subjects; underestimate fat mass in very lean subjects) | Inconsistent clothing worn during assessment |
| Inconsistent subject positioning (prone vs. supine) | Changing software platforms |
General Margin of Error
Although DXA has been reported to accurately measured body fat percentage within 1% margin of error compared with a four-compartment model in ethnically diverse male and female athletes from various sporting backgrounds [36], DXA typically has a 2-3% standard error estimate (SEE) when predicting body fat percentage [37].
The standardization of body composition assessment is the most critical aspect for accurate result interpretation and quantification, and must not be overlooked [38]. To minimize preventable error when using DXA to assess body composition, I advise utilizing the best-practice protocol outlined by Nana et al. (2015), [20].
This research group also provides a nice list of advantages and disadvantages for practically using DXA with athletes:
| Advantages | Disadvantages |
| Suitable for most athletes | Expensive equipment |
| Fast (~5 mins for fan beam, up to 15 mins for pencil beam) | Generally not portable |
| Provides regional body composition | Most scanning beds too small for typical physique of larger athletes |
| Radiation dose is low dose (~0.5 µSv) and safe for sequential measurements | Trained technician required |
| Non-intrusive | Manufacturers’ body composition algorithms may not be appropriate for athletic population |
Summary
Dual energy X-ray absorptiometry (DXA) is one of the most widely used body composition assessment methods available, and for good reason. It’s non-intrusive, extremely precise, and enables for regional body composition assessment, including bone mass. However, it’s also expensive, emits a small dose of radiation with each use, requires a technician to operate, and is, generally, not portable. Various factors affect its accuracy and reliability, including previous exercise, hydration, and eating habits. As is the case with any body composition assessment method, understanding the factors that affect the accuracy and reliability of DXA, and applying a standardized approach for data collection is advised to avoid measurement artifact caused by these factors. In any case, the most important aspect of body composition assessment is the standardization of data collection. If standardization is lacking, misinterpretation of athlete physique is near-definite [38].
Enjoying the Content?
Instantly become an important part of the Shakebot community by connecting with me on social media:




References
- Buckinx, F., Landi, F., Cesari, M., Fielding, R.A., Visser, M., Engelke, K., Maggi, S., Dennison, E., Al?Daghri, N.M., Allepaerts, S. and Bauer, J., 2018. Pitfalls in the measurement of muscle mass: a need for a reference standard. Journal of Cachexia, Sarcopenia and Muscle.
- Erlandson, M.C., Lorbergs, A.L., Mathur, S. and Cheung, A.M., 2016. Muscle analysis using pQCT, DXA and MRI. European Journal of Radiology, 85(8), pp.1505-1511.
- Bosch, T.A., Carbuhn, A., Stanforth, P.R., Oliver, J.M., Keller, K.A. and Dengel, D.R., 2017. Body composition and bone mineral density of division 1 collegiate football players, a consortium of college athlete research (C-CAR) study. Journal of Strength and Conditioning Research.
- Fornetti, W.C., Pivarnik, J.M., Foley, J.M. and Fiechtner, J.J., 1999. Reliability and validity of body composition measures in female athletes. Journal of Applied Physiology, 87(3),pp.1114-1122.
- Wang, J.G., Zhang, Y., Chen, H.E., Li, Y., Cheng, X.G., Xu, L., Guo, Z., Zhao, X.S., Sato, T., Cao, Q.Y. and Chen, K.M., 2013. Comparison of two bioelectrical impedance analysis devices with dual energy X-ray absorptiometry and magnetic resonance imaging in the estimation of body composition. The Journal of Strength & Conditioning Research, 27(1),pp.236-243.
- Prior, B.M., Cureton, K.J., Modlesky, C.M., Evans, E.M., Sloniger, M.A., Saunders, M. and Lewis, R.D., 1997. In vivo validation of whole body composition estimates from dual-energy X-ray absorptiometry. Journal of Applied Physiology, 83(2),pp.623-630.
- Wang, Z., Heymsfield, S.B., Chen, Z., Zhu, S.and Pierson, R.N., 2010. Estimation of percentage body fat by dual-energy x-ray absorptiometry: evaluation by in vivo human elemental composition. Physics in Medicine & Biology, 55(9), p.2619.
- Meyer, N.L., Sundgot-Borgen, J., Lohman, T.G., Ackland, T.R., Stewart, A.D., Maughan, R.J., Smith, S. and Müller, W., 2013. Body composition for health and performance: a survey of body composition assessment practice carried out by the Ad Hoc Research Working Group on Body Composition, Health and Performance under the auspices of the IOC Medical Commission. Br J Sports Med, pp.bjsports-2013.
- López-Taylor, J.R., González-Mendoza, R.G.,Gaytán-González, A., Jiménez-Alvarado, J.A., Villegas-Balcázar, M., Jáuregui-Ulloa, E.E. and Torres-Naranjo, F., 2018. Accuracy of anthropometric equations for estimating body fat in professional male soccer players compared with DXA. Journal of Sports Medicine, 2018.
- Reilly, T., George, K., Marfell-Jones, M., Scott, M., Sutton, L. and Wallace, J.A., 2009. How well do skinfold equations predict percent body fat in elite soccer players?. International Journal of Sports Medicine, 30(08), pp.607-613.
- Oliver, J.M., Lambert, B.S., Martin, S.E., Green, J.S. and Crouse, S.F., 2012. Predicting football players’ dual-energy x-ray absorptiometry body composition using standard anthropometric measures. Journal of Athletic Training, 47(3), pp.257-263.
- Ball, S.D., Altena, T.S. and Swan, P.D., 2004. Comparison of anthropometry to DXA: a new prediction equation for men. European Journal of Clinical Nutrition, 58(11), p.1525.
- Garcia, A.L., Wagner, K., Hothorn, T.,Koebnick, C., Zunft, H.J.F. and Trippo, U., 2005. Improved prediction of body fat by measuring skinfold thickness, circumferences, and bone breadths. Obesity, 13(3),pp.626-634.
- Duz, S., Kocak, M. and Korkusuz, F., 2009. Evaluation of body composition using three different methods compared todual-energy X-ray absorptiometry. European Journal of Sport Science, 9(3),pp.181-190.
- Moon, J.R., Eckerson, J.M., Tobkin, S.E., Smith, A.E., Lockwood, C.M., Walter, A.A., Cramer, J.T., Beck, T.W. and Stout, J.R., 2009. Estimating body fat in NCAA Division I female athletes: a five-compartment model validation of laboratory methods. European Journal of Applied Physiology, 105(1), pp.119-130.
- Fosbøl, M.Ø. and Zerahn, B., 2015. Contemporary methods of body composition measurement. Clinical Physiology and Functional Imaging, 35(2), pp.81-97.
- Thomsen, T.K., Jensen, V.J. and Henriksen, M.G., 1998. In vivo measurement of human body composition by dual-energy X-ray absorptiometry (DXA). The European Journal of Surgery, 164(2),pp.133-137.
- Horber, F.F., Thomi, F., Casez, J.P.,Fonteille, J. and Jaeger, P.H., 1992. Impact of hydration status on body composition as measured by dual energy X-ray absorptiometry in normal volunteers and patients on haemodialysis. The British Journal of Radiology, 65(778), pp.895-900.
- Nana, A., Slater, G.J., Hopkins, W.G. and Burke, L.M., 2012. Effects of daily activities on dual-energy X-ray absorptiometry measurements of body composition in active people. Medicine & Science in Sports & Exercise, 44(1), pp.180-189.
- Nana, A., Slater, G.J., Stewart, A.D. and Burke, L.M., 2015. Methodology review: using dual-energy X-ray absorptiometry (DXA) for the assessment of body composition in athletes and active people. International Journal of Sport Nutrition and Exercise Metabolism, 25(2), pp.198-215.
- Bone, J.L., Ross, M.L., Tomcik, K.A., Jeacocke, N.A., Hopkins, W.G. and Burke, L.M., 2017. Manipulation of muscle creatine and glycogen changes dual X-ray absorptiometry estimates of body composition. Medicine & Science in Sports & Exercise, 49(5), pp.1029-1035.
- Rouillier, M.A., David-Riel, S., Brazeau, A.S.,St-Pierre, D.H. and Karelis, A.D., 2015. Effect of an acute high carbohydrate diet on body composition using DXA in young men. Annals of Nutrition and Metabolism, 66(4), pp.233-236.
- Safdar, A., Yardley, N.J., Snow, R., Melov, S.and Tarnopolsky, M.A., 2008. Global and targeted gene expression and protein content in skeletal muscle of young men following short-term creatine monohydrate supplementation. Physiological Genomics, 32(2),pp.219-228.
- Pietrobelli, A., Wang, Z., Formica, C. and Heymsfield, S.B., 1998. Dual-energy X-ray absorptiometry: fat estimation errors due to variation in soft tissue hydration. American Journal of Physiology-Endocrinology And Metabolism, 274(5), pp.E808-E816.
- Lambrinoudaki, I., Georgiou, E., Douskas, G.,Tsekes, G., Kyriakidis, M. and Proukakis, C., 1998. Body composition assessment by dual-energy x-ray absorptiometry: comparison of prone and supine measurements. Metabolism, 47(11), pp.1379-1382.
- Lohman, M., Tallroth, K., Kettunen, J.A. and Marttinen, M.T., 2009. Reproducibility of dual-energy x-ray absorptiometry total and regional body composition measurements using different scanning positions and definitions of regions. Metabolism-Clinical and Experimental, 58(11), pp.1663-1668.
- Pritchard, J.E., Nowson, C.A., Strauss, B.J., Carlson, J.S., Kaymakci, B. and Wark, J.D., 1993. Evaluation of dual energy X-ray absorptiometry as a method of measurement of body fat. European Journal of Clinical Nutrition, 47(3), pp.216-228.
- Soriano, J.M.P., Ioannidou, E., Wang, J., Thornton, J.C., Horlick, M.N., Gallagher, D., Heymsfield, S.B. and Pierson Jr, R.N., 2004. Pencil-beam vs fan-beam dual-energy X-ray absorptiometry comparisons across four systems: body composition and bone mineral. Journal of Clinical Densitometry, 7(3), pp.281-289.
- Tothill, P., Hannan, W.J. and Wilkinson, S., 2001. Comparisons between a pencil beam and two fan beam dual energy X-ray absorptiometers used for measuring total body bone and soft tissue. The British Journal of Radiology, 74(878), pp.166-176.
- Guo, Y., Franks, P.W., Brookshire, T. and Tataranni, P.A., 2004. The intra?and inter?instrument reliability of DXA based on ex vivo soft tissue measurements. Obesity, 12(12),pp.1925-1929.
- Clasey, J.L., Hartman, M.L., Kanaley, J., Wideman, L.A.U.R.I.E., Teates, C.D., Bouchard, C. and Weltman, A., 1997. Body composition by DEXA in older adults: accuracy and influence of scan mode. Medicine and Science in Sports and Exercise, 29(4), pp.560-567.
- Hull, H., He, Q., Thornton, J., Javed, F., Allen, L., Wang, J., Pierson, R.N. and Gallagher, D., 2009. iDXA, Prodigy, and DPXL dual-energy X-ray absorptiometry whole-body scans: a cross-calibration study. Journal of Clinical Densitometry, 12(1),pp.95-102.
- Kistorp, C.N. and Svendsen, O.L., 1998. Body composition results by DXA differ with manufacturer, instrument generation and software version. Applied Radiation and Isotopes, 49(5-6),pp.515-516.
- Van Loan, M.D., Keim, N.L., Berg, K. andMayclin, P.L., 1995. Evaluation of body composition by dual energy x-ray absorptiometry and two different software packages. Medicine and Science in Sports and Exercise, 27(4), pp.587-591.
- Bilsborough, J.C., Greenway, K., Opar, D., Livingstone, S., Cordy, J. and Coutts, A.J., 2014. The accuracy and precision of DXA for assessing body composition in team sport athletes. Journal of Sports Sciences, 32(19), pp.1821-1828.
- Deurenberg, P., Weststrate, J.A. and Paymans, I., 1988. Factors affecting bioelectrical impedance measurements in humans. European Journal of Clinical Nutrition, 42(12),pp.1017-1022.
- Ackland, T.R., Lohman, T.G., Sundgot-Borgen,J., Maughan, R.J., Meyer, N.L., Stewart, A.D. and Müller, W., 2012. Current status of body composition assessment in sport. Sports Medicine, 42(3),pp.227-249.
- Kerr, A.D., Slater, G.J. and Byrne, N.M., 2018. Influence of subject presentation on interpretation of body composition change after 6 months of self-selected training and diet in athletic males. European Journal of Applied Physiology, 118(6), pp.1273-1286.