Monitoring body composition in athletes is beneficial for a myriad of reasons. BIA, or bioelectrical impedance analysis, is one of many methods that can be used to assess body composition in athletes. How BIA works, its popularity, and common sources and margin of error are reviewed in this article.
Grey boxes are summary points
Blue boxes give more detail about key terms or subjects
How BIA Works
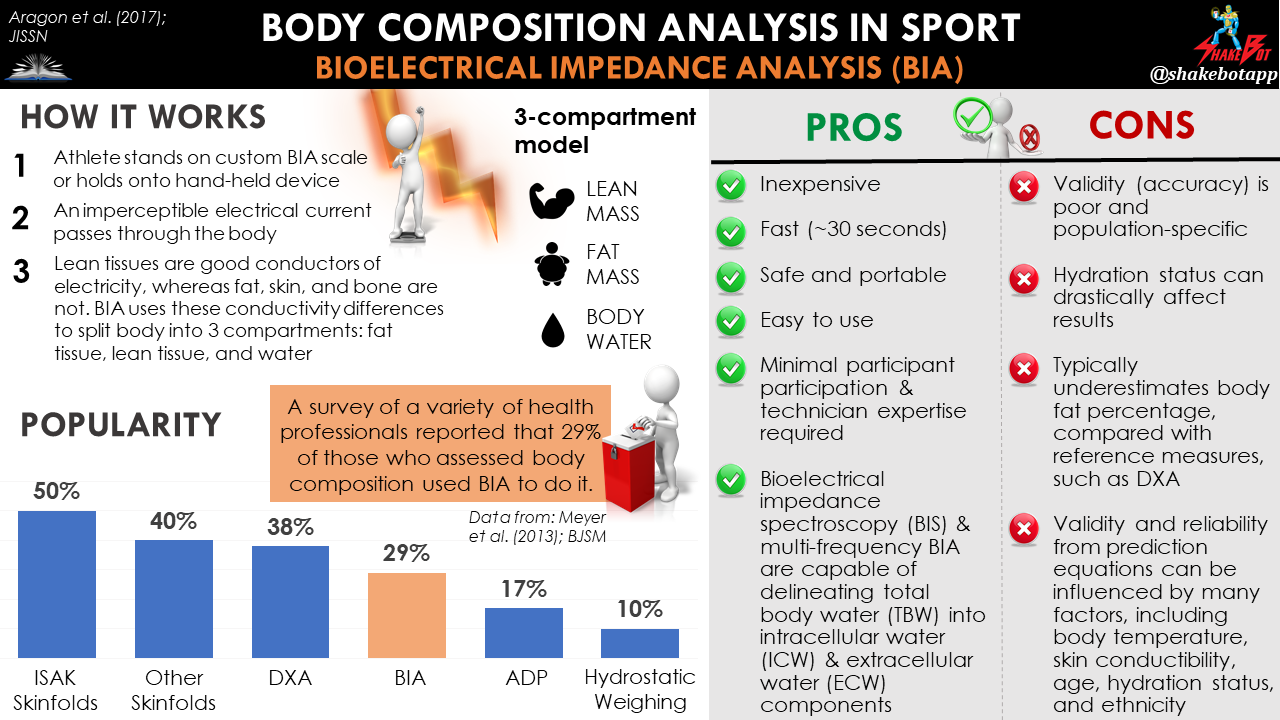
Bioelectrical impedance analysis (BIA) is based on the electrical conductive properties of the human body [1]. Using an imperceptible electrical current passed through the body, BIA segregates the body into 3 compartments: fat tissue, lean tissue, and water [1]. Lean tissues are good conductors of electrical current due to their large amount of water and electrolytes (i.e. they show low resistance to passage of electrical current). In contrast, fat, bone, and skin have low conductivity and are poor conductors of electrical current due to their small quantity of fluid and electrolytes (i.e. they show high resistance to passage of electrical current). BIA uses these differences in resistance to the flow of electrical current through the body to estimate body composition [2].
The harmless electrical current starts from point A which is, generally, an arm or a leg. When the current finally reaches its endpoint, generally another arm or a leg, it will have lost some of its voltage on its journey through body water. From there, the impedance (resistance) is determined, and body composition is estimated.
BIA = Bioelectrical impedance analysis. A method for body composition assessment that sends an imperceptible electrical current through the body. The conductivity differences among bodily tissues allows BIA to predict the breakdown of (1) lean mass, (2) fat mass, and (3) body water.
Popularity
BIA is one of the most widely utilized techniques for measuring body composition, with 29% of national and international sport professionals reporting its use for body composition assessment, in a 2013 survey [3]. BIA was particularly popular in Europe, where it was the 2nd-most popular method for body composition assessment. Skinfold measurements came in at #1, with 47-50% of European sport professionals utilizing this method, followed by BIA at 42% and, then, DXA at 35% [3]. BIA was not nearly as popular in the Americas or Oceania, with 15% and 14% of professionals reporting its use, respectively [3]. Despite its lack of validity in athletes [3], its safety, affordability, and speed of data collection make BIA a practical body composition assessment option in the applied sports setting [4].

Aragon et al. (2017). International society of sports nutrition position stand: diets and body composition. Journal of the International Society of Sports Nutrition, 14(1), p.16.
Let’s Talk Frequency
When BIA sends the (harmless) electrical current through the body, both the device and method used determine the frequency, or frequencies, of conduction [5]. BIA has been performed using single-frequency (SF-BIA) or multiple-frequency (MF-BIA) electrical current. Standard SF-BIA uses a single frequency of 50 kHz to estimate total body water and fat-free mass, but cannot differentiate between the water that is inside of cells (intracellular water; ICW) and the water outside of cells (extracellular water; ECW). This is because, at low frequencies (< 50 kHz), the electrical current cannot pass through cell membranes and, therefore, can only predict water concentrations outside of cells (i.e. extracellular water; ECW). However, at higher frequencies (>50 kHz), the electrical current can penetrate cell membranes and be used to estimate intracellular water volumes [5].
BIS = Bioelectrical spectroscopy. A version of bioelectrical impedance analysis (BIA) that sends multiple, or a “spectra”, of electrical current frequencies for body composition prediction. Using multiple frequencies allows for estimated differences between intracellular and extracellular water compartments in the body.
In general, multi-frequency BIA (MF-BIA) does not improve the estimate of body composition compared to SF-BIA, but it’s advantageous in that it also estimates ICW and ECW by measuring the body’s resistance to a spectrum of frequencies [2, 6]. You will also see the term “BIS”, or “bioelectrical spectroscopy”, which refers to the same concept as MF-BIA. In other words, both multi-frequency BIA (MF-BIA) and bioelectrical spectroscopy (BIS) send out electrical current at multiple, or a “spectra” of, frequencies to estimate body composition. Single-frequency BIA (SF-BIA) only sends out current at a single frequency.
The basic principle that lays the foundation for BIA is the notion that only certain tissues can be penetrated by specific frequencies of electrical current [7]. Regardless of the device or method used, there are three key assumptions that BIA/BIS make when estimating body composition: (1) the conductor (i.e. body) is shaped like a uniform cylinder, (2) the electrical current is distributed uniformly throughout the conductor (i.e. body), and (3) the body contains 72.3% water [2].
The contributors to the InBody website provide graphics which do a great job of detailing the limitations of these assumptions; you can view their insights here (I have no affiliation with InBody in any capacity).
The Different Types of Devices
There are many different BIA devices out there, with the most popular being hand-to-hand (i.e. handheld), foot-to-foot (i.e. standing scale), hand-to-foot or “whole body” (i.e. adhesive electrodes or scale-handheld combo), and direct segmental (i.e. modern method using advanced technology).

Hand-to-Hand
- Typically involves using a handheld device
- Assumes body is in the shape of a single, uniform cylinder
- Only measures impedance of upper body/arms, and estimates the trunk and leg compartments through prediction equations
- These devices predict your overall body composition based on the estimated composition of your arms
Foot-to-Foot
- Typically involves standing on a scale
- Assumes body is in the shape of a single, uniform cylinder
- Only measures impedance of the legs, and estimates the trunk and upper body compartments through prediction equations
- These devices predict your overall body composition based on the estimated composition of your legs
Foot-to-Hand (“Whole Body”)
- Typically involves standing on a scale and holding onto a conductive device with your hands
- Assumes body is in the shape of a single, uniform cylinder
- Some devices only measure one side of the body and estimate the other side (or parts of it)
- Some devices measure the left and right sides of the body and estimate the trunk (or parts of it)
- These devices typically predict your overall body composition based on the estimated composition of one side of the body
Direct Segmental
- Typically involves standing on a scale and holding onto a conductive device with your hands
- Assumes body is in the shape of 5 discrete cylinders (2 arms, 2 legs, 1 trunk)
- Uses direct impedance measurements from the various body compartments (the 5 “cylinders”)
- Typically uses multiple frequencies (the InBody 720 uses 6: 1 kHz, 5 kHz, 50 kHz, 250 kHz, 500 kHz, 1000 kHz)
- These devices predict your overall body composition based on the estimated composition of the trunk, each arm, and each leg
The Precision Issue
Although many BIA equations have been investigated [8], its accuracy/validity for estimating total body water and fatness is limited, particularly in athletes and trained individuals. BIA prediction inaccuracy typically sits between the 2-3% to 5-6% range, when compared with the most accurate assessment methods [9-13, 15-21]. Although this is not always the case, BIA tends to underestimate the body fat percentage; it gives lower values, compared with more precise methods. It’s also important to note that the error in precision tends to increase in individuals with higher body fat percentages [13, 21].
In a comparison between BIA and dual energy x-ray absorptiometry (DXA) for assessment of total and regional body composition in healthy young adults, there was a small, although statistically significant, 4% difference between the two methods [13]. Schoenfeld et al. (2018) reported a much smaller discrepancy between BIA (InBody 720) and DXA [14]. In 21 resistance-trained men, BIA overestimated body fat percentage by ~1.2%, compared with DXA [14]. In contrast, Ferri-Morales et al. (2018) found large body composition differences between BIA, air displacement plethysmography (ADP; BOD POD), and DXA measurements in 104 young male athletes [21]. Compared with DXA and ADP, BIA underestimated body fat percentage by 2.0% and 5.3%, respectively [21]. In a careful comparison between BIA and skinfold measurements in wrestlers, both methods predicted body fat percentage with a standard error estimate (SEE) of 3.5%, compared with densitometry, a body composition assessment method with well-documented high precision [15]. Montogomery et al. (2017) compared four different BIA devices with ADP (BOD POD) in 134 young American wrestlers [12]. Compared with BOD POD, the four different BIA devices underestimated body fat percentage by 0.7%, 2.2%, 2.5%, and 3.6% [12].
DXA = Dual energy x-ray absorptiometry. Passes filtered x-ray beams with two different photon energies (emitting a very small dose of ionizing radiation) through the body to produce pictures of the inside of the body, and is considered one of the “gold standard” methods for body composition assessment. DXA can estimate the breakdown of (1) lean mass, (2) fat mass, and (3) bone mineral content, by body segment, because each tissue differentiates photons differently.
ADP = Air displacement plethysmography. The subject is required to sit inside an enclosed chamber (plethysmograph), most commonly measured via a device called the BOD POD, and is considered another “gold standard” method for body composition assessment. It estimates the subject’s body volume from the air that gets displaced when the subject is in the chamber, and using Boyle’s law (and the Siri equation), ADP estimates the breakdown of (1) lean mass, and (2) fat mass, inside the body.

Even the most robust BIA devices today can have substantial degrees of error. For example, Mala et al. (2016) found that BIA direct segmental analyzers (BIA 2000M and InBody 3.0) overestimated body fat percentage in elite female soccer players by ~4% and ~6%, respectively, compared with hydrodensitometry [16]. This is an atypical result for BIA assessment, as it generally underestimates body fat percentage. In 45 college female athletes, Esco et al. (2015) reported that the multi-frequency BIA device InBody 720 (another direct segmental device) underestimated body fat percentage by 3.3%, compared with DXA [5]. Similarly, in a study by Raymond et al. (2018), multi-frequency BIA using the InBody 770 underestimated body fat percentage by 3%, compared with DXA, in 44 NCAA Division 1 football players [17]. Using the Tanita BC-418, another segmental body composition analyzer, BIA has underestimated body fat percentage in elite lean soccer players by 2-3% [18, 19]. In a mixed cohort of 33 male elite ice hockey and soccer athletes, Svantesson et al. (2008) reported that BIA (using BIS / multi-frequency BIA) underestimated body fat percentage by 2.8%, compared with DXA [20].
The inaccuracies of BIA for estimating body composition can be, at times, dramatic. In 396 Brazilian male army cadets, Langer et al. (2016) reported that some individuals could have their fat-free mass (FFM) values overestimated by more than nine kilograms, and underestimated by more than eight kilograms, compared with DXA [21]. These overestimation and underestimation values would correspond to errors of 16% and 14%, respectively [21]. These data speak toward the wide range of error-prone outcomes that can result from BIA, regardless of the method and device used.
| Biological Sources of Error | Technical Sources of Error |
| Hydration status | Changing BIA device manufacturer or change in product specs |
| Body temperature and perspiration | Single-frequency vs. Multi-frequency vs. Bioelectrical spectroscopy (BIS) |
| Acute food and fluid intake | Placement and positioning of electrodes on the skin |
| Changes in body size and shape | Machine type (hand-hand vs. foot-foot vs. “whole body” vs. direct segmental) |
Improving Reliability
Although the aforementioned research suggests questionable precision, the accuracy of BIA can be enhanced by selecting a regression equation suitable for the demographic being assessed (i.e. in our case, athletes), [1, 20, 22, 23]. Many factors, including those related to the device being used (i.e. intra-instrumental and inter-instrumental variability, electrode quality, and electrode positioning), prediction equation, technician (i.e. intra-operator and inter-operator variability), subject/athlete (i.e. subject preparation such as position, overnight fast or empty bladder, body temperature, skin conductibility, age, hydration status, and ethnicity), and environment (i.e. ambient temperature), can add significant variance to the BIA assessment results [20, 24-29, 34].
Perhaps the biggest challenge with BIA reliability is hydration status [28]. Saunders et al. (1998) concluded that BIA was not valid in athletes with abnormal hydration status, such as being hypohydrated, rehydrated or superhydrated [30]. Although lacking validity, the consistency/reliability of BIA has been reported to be quite good [14, 30, 31], particularly when steps are taken to standardize conditions between measurements [1, 14, 33-35].
Regardless of the technology or method used, adopting a standardized approach is crucial for identifying valid alterations in body composition. With BIA in particular, standardization, or control over as many relevant factors as possible, is essential for minimizing error because of the extreme effects that these many different factors (especially hydration) can have on the results. If adopting BIA to assess body composition, it would be wise to review the standardization guidelines presented by Kyle et al. (2004), to optimize validity and reliability [25].
Common advantages and disadvantages of using BIA for body composition assessment are provided by Aragon et al. (2017), and are summarized below [4]:
| Advantages | Disadvantages |
| Low cost | Poor precision |
| Safe | Validity and reliability can be influenced by many factors, including sex, age, height, disease state, and race |
| Quick to execute (~30 seconds for most devices) | Hydration status drastically affects validity and reliability |
| Minimal participant participation required | Typically underestimates body fat percentage in normal-weight individuals and athletes, compared with DXA |
| Capable of determining total body water (and intracellular & extracellular water components, depending on the device) | Validity of single-frequency BIA and multifrequency BIA may be limited to healthy, young, euhydrated adults. |
Summary
Bioelectrical impedance analysis (BIA) is a safe, non-invasive way to estimate longitudinal changes in body composition in athletes, but also has several hurdles that must be overcome in order to obtain reliable results, with the major culprit being hydration status. Although it’s inexpensive and quick to execute, the precision is poor, and various factors must be controlled to accurately assess the body composition changes that occur over time. As is the case with any body composition assessment method, understanding the factors that affect the accuracy and reliability of BIA, and applying a standardized approach for data collection, is advised in order to avoid measurement artifact caused by these factors.
In any case, the most important aspect of body composition assessment is the standardization of data collection. If standardization is lacking, misinterpretation of athlete physique is near-definite [37].
References
- Fosbøl, M.Ø. and Zerahn, B., 2015. Contemporary methods of body composition measurement. Clinical Physiology and Functional Imaging, 35(2), pp.81-97.
- Mialich, M.S., Sicchieri, J.F. and Junior,A.A.J., 2014. Analysis of body composition: a critical review of the use of bioelectrical impedance analysis. Int J Clin Nutr, 2(1),pp.1-10.
- Meyer, N.L., Sundgot-Borgen, J., Lohman, T.G., Ackland, T.R., Stewart, A.D., Maughan, R.J., Smith, S. and Müller, W., 2013. Body composition for health and performance: a survey of body composition assessment practice carried out by the Ad Hoc Research Working Group on Body Composition, Health and Performance under the auspices of the IOC Medical Commission. Br J Sports Med, pp.bjsports-2013.
- Aragon, A.A., Schoenfeld, B.J., Wildman, R., Kleiner, S., VanDusseldorp, T., Taylor, L., Earnest, C.P., Arciero, P.J., Wilborn, C., Kalman, D.S. and Stout, J.R., 2017. International society of sports nutrition position stand: diets and body composition. Journal of the International Society of Sports Nutrition, 14(1), p.16.
- Esco, M.R., Snarr, R.L., Leatherwood, M.D., Chamberlain, N.A., Redding, M.L., Flatt, A.A., Moon, J.R. and Williford, H.N., 2015. Comparison of total and segmental body composition using DXA and multifrequency bioimpedance in collegiate female athletes. The Journal of Strength &Conditioning Research, 29(4), pp.918-925.
- Castizo-Olier, J., Irurtia, A., Jemni, M., Carrasco-Marginet, M., Fernández-García, R. and Rodríguez, F.A., 2018. Bioelectrical impedance vector analysis (BIVA) in sport and exercise: Systematic review and future perspectives. PloS One, 13(6), p.e0197957.
- Moon, J.R., 2013. Body composition in athletes and sports nutrition: an examination of the bioimpedance analysis technique. European Journal of Clinical Nutrition, 67(S1), p.S54.
- Kyle, U.G., Bosaeus, I., De Lorenzo, A.D., Deurenberg, P., Elia, M., Gómez, J.M., Heitmann, B.L., Kent-Smith, L., Melchior, J.C., Pirlich, M. and Scharfetter, H., 2004. Bioelectrical impedance analysis—part I: review of principles and methods. Clinical Nutrition, 23(5),pp.1226-1243.
- Jackson, A.S., Pollock, M.L., Graves, J.E. and Mahar, M.T., 1988. Reliability and validity of bioelectrical impedance in determining body composition. Journal of Applied Physiology, 64(2),pp.529-534.
- Shim, A., Cross, P., Norman, S. and Hauer, P., 2014. Assessing various body composition measurements as an appropriate tool for estimating body fat in National Collegiate Athletic Association Division I female collegiate athletes. American Journal of Sports Science and Medicine, 2(1), pp.1-5.
- Merrigan, J., Gallo PhD, S., Fields, J. and Jones PhD, M.T., 2018. Foot-to-foot bioelectrical impedance, air displacement plethysmography, and dual energy x-ray absorptiometry in resistance-trained men and women. International Journal of Exercise Science, 11(4), pp.1145-1155.
- Montgomery, M.M., Marttinen, R.H. and Galpin, A.J., 2017. Comparison of body fat results from 4 bioelectrical impedance analysis devices vs. air displacement plethysmography in American adolescent wrestlers. International Journal of Kinesiology and Sports Science, 5(4), pp.18-25.
- Leahy, S., O’Neill, C., Sohun, R. and Jakeman, P., 2012. A comparison of dual energy X-ray absorptiometry and bioelectrical impedance analysis to measure total and segmental body composition in healthy young adults. European Journal of Applied Physiology, 112(2),pp.589-595.
- Schoenfeld, B.J., Nickerson, B.S., Wilborn, C.D., Urbina, S.L., Hayward, S.B., Krieger, J., Aragon, A.A. and Tinsley, G.M., 2018. Comparison of multifrequency bioelectrical impedance vs. dual-energy x-ray absorptiometry for assessing body composition changes after participation in a 10-week resistance training program. Journal of Strength and Conditioning Research.
- Lohman, T.G., 1992. Advances in body composition assessment. Human Kinetics, pp.1-23.
- Mala, L., Maly, T., Zahalka, F., Cabell, L. and Bonacin, D., 2016. A comparison of methods for evaluating body composition in elite female soccer players. The Anthropologist, 24(2),pp.642-651.
- Raymond, C.J., Dengel, D.R. and Bosch, T.A., 2018. Total and segmental body composition examination in collegiate football players using multifrequency bioelectrical impedance analysis and dual x-ray absorptiometry. The Journal of Strength & Conditioning Research, 32(3),pp.772-782.
- Leão, C., Simões, M., Silva, B., Clemente, F.M., Bezerra, P. and Camões, M., 2017. Body composition evaluation issue among young elite football players: DXA assessment. Sports, 5(1),p.17.
- Lozano Berges, G., Matute Llorente, Á., Gómez Bruton, A., González Agüero, A., Rodríguez, G.V. and Casajús, J.A., 2017. Body fat percentage comparisons between four methods in young football players: are they comparable?. Nutricion Hospitalaria, 34(5).
- Svantesson, U., Zander, M., Klingberg, S. and Slinde, F., 2008. Body composition in male elite athletes, comparison of bioelectrical impedance spectroscopy with dual energy X-ray absorptiometry. Journal of Negative Results in Biomedicine, 7(1),p.1.
- Ferri-Morales, A., Nascimento-Ferreira, M.V., Vlachopoulos, D., Ubago-Guisado, E., Torres-Costoso, A., De Moraes, A.C.F., Barker, A.R., Moreno, L.A., Martínez-Vizcaino, V. and Gracia-Marco, L., 2018. Agreement between standard body composition methods to estimate percentage of body fat in young male athletes. Pediatric Exercise Science, 20(XX), pp.1-9.
- Langer, R.D., Borges, J.H., Pascoa, M.A.,Cirolini, V.X., Guerra-Júnior, G. and Gonçalves, E.M., 2016. Validity of bioelectrical impedance analysis to estimation fat-free mass in the army cadets. Nutrients, 8(3), p.121.
- Buchholz, A.C., Bartok, C. and Schoeller, D.A., 2004. The validity of bioelectrical impedance models in clinical populations. Nutrition in Clinical Practice, 19(5),pp.433-446.
- Ellis, K.J., Bell, S.J., Chertow, G.M.,Chumlea, W.C., Knox, T.A., Kotler, D.P., Lukaski, H.C. and Schoeller, D.A., 1999. Bioelectrical impedance methods in clinical research: a follow-up to the NIH Technology Assessment Conference. Nutrition, 15(11),pp.874-880.
- Buckinx, F., Landi, F., Cesari, M., Fielding,R.A., Visser, M., Engelke, K., Maggi, S., Dennison, E., Al?Daghri, N.M., Allepaerts, S. and Bauer, J., 2018. Pitfalls in the measurement of muscle mass: a need for a reference standard. Journal of Cachexia, Sarcopeniaand Muscle.
- Kyle, U.G., Bosaeus, I., De Lorenzo, A.D., Deurenberg, P., Elia, M., Gómez, J.M., Heitmann, B.L., Kent-Smith, L.,Melchior, J.C., Pirlich, M. and Scharfetter, H., 2004. Bioelectrical impedance analysis—part II: utilization in clinical practice. Clinical Nutrition, 23(6),pp.1430-1453.
- Deurenberg, P., Weststrate, J.A. and Paymans, I., 1988. Factors affecting bioelectrical impedance measurements in humans. European Journal of Clinical Nutrition, 42(12),pp.1017-1022.
- Backes, T.P., Swartz, C., Conti, A. and Knapp, J.M., 2017. The effect of fluid consumption and exercise on segmental bioelectrical impedance. International Journal of Physical Education, Fitness and Sports, 6(2), pp.10-13.
- Gudivaka, R., Schoeller, D.A.L.E. and Kushner, R.F., 1996. Effect of skin temperature on multifrequency bioelectrical impedance analysis. Journal of Applied Physiology, 81(2), pp.838-845.
- Slater, G., Shaw, G. and Kerr, A., 2018. Athlete Considerations for Physique Measurement. In Best Practice Protocols for Physique Assessment in Sport (pp. 47-60). Springer, Singapore.
- Saunders, M.J., Blevins, J.E. and Broeder, C.E., 1998. Effects of hydration changes on bioelectrical impedance in endurance trained individuals. Medicine and Science in Sports and Exercise, 30(6),pp.885-892.
- Hurst, P.R., Walsh, D.C., Conlon, C.A., Ingram,M., Kruger, R. and Stonehouse, W., 2016. Validity and reliability of bioelectrical impedance analysis to estimate body fat percentage against air displacement plethysmography and dual?energy X?ray absorptiometry. Nutrition & Dietetics, 73(2), pp.197-204.
- Tinsley, G.M., 2018. Reliability and agreement between DXA-derived body volumes and their usage in 4-compartment body composition models produced from DXA and BIA values. Journal of Sports Sciences, 36(11), pp.1235-1240.
- Bosquet, L., Niort, T. and Poirault, M., 2017. Intra-and inter-day reliability of body composition assessed by a commercial multifrequency bioelectrical impedance meter. Sports Medicine International Open, 1(04), pp.E141-E146.
- Kerr, A., Slater, G.J. and Byrne, N., 2017. Impact of food and fluid intake on technical and biological measurement error in body composition assessment methods in athletes. British Journal of Nutrition, 117(4), pp.591-601.
- Lukaski, H.C., Bolonchuk, W.W., Siders, W.A.and Hall, C.B., 1990. Body composition assessment of athletes using bioelectrical impedance measurements. J Sports Med Phys Fitness, 30(4),pp.434-440.
- Kerr, A.D., Slater, G.J. and Byrne, N.M., 2018. Influence of subject presentation on interpretation of body composition change after 6 months of self-selected training and diet in athletic males. European Journal of Applied Physiology, 118(6), pp.1273-1286.